
Young eyes are not small adult eyes. A ten-year-old’s crystalline lens passes approximately 85–90% of incoming blue light at 480 nm directly to the retina — where the ipRGC photoreceptors that suppress melatonin are waiting. An adult at forty transmits roughly 70%. That gap alone makes children a higher-sensitivity population for ALAN-driven circadian disruption. Add the two-hour phase delay that puberty programs into the adolescent chronotype, and you have a double hit: biology pulling the clock later while screen-based ALAN holds it there. The result is Delayed Sleep-Wake Phase Disorder (DSPD) affecting an estimated 7 to 16% of adolescents, compared to 0.17% of the general adult population. For the full mechanistic picture of how light suppresses melatonin, see light pollution and human health: the science of darkness, disrupted.
Why Children’s Eyes Are More Vulnerable
The clearer the lens, the more blue photons reach the ipRGCs — and in children under twelve, the lens is nearly transparent to the wavelengths that matter most.
The human crystalline lens yellows progressively across a lifetime. Chromophores accumulate in the lens matrix, absorbing short-wavelength light before it reaches the retina. This is not a pathology. It is normal ageing physiology — but its consequences for circadian biology are substantial.
Kessel and colleagues (2011, Ophthalmic Research, vol. 46, pp. 118–124) quantified the rate of change in blue-light transmission at 480 nm — the wavelength peak of melanopsin sensitivity in ipRGCs — across the human lifespan. Their finding: lens transmission at 480 nm declines by approximately 0.7 to 0.8% per year. Across the span from age ten to age eighty, that compounds to a reduction of roughly 49 to 56% in the photons reaching the retina. A child at ten is transmitting roughly 85 to 90% of incoming 480 nm light to ipRGCs. An adult at forty transmits approximately 70%. By eighty, fewer than 45% get through.
The implication is direct. Identical screen exposure — same device, same brightness, same CCT — delivers substantially more melanopsin-activating photons to a child’s retina than to an adult’s. Melatonin suppression per lux of screen output is higher in children. The pre-sleep circadian phase shift per hour of screen use is larger. Yet screen time recommendations and bedroom light standards are rarely designed to account for this spectral asymmetry. For a detailed account of the ipRGC-to-pineal signal pathway these photons activate, see melatonin and the ipRGC-to-pineal pathway.
The Adolescent Chronotype Shift
Puberty re-programmes the circadian clock. It is not laziness — it is developmental neurobiology, and it runs on a two-hour delay.

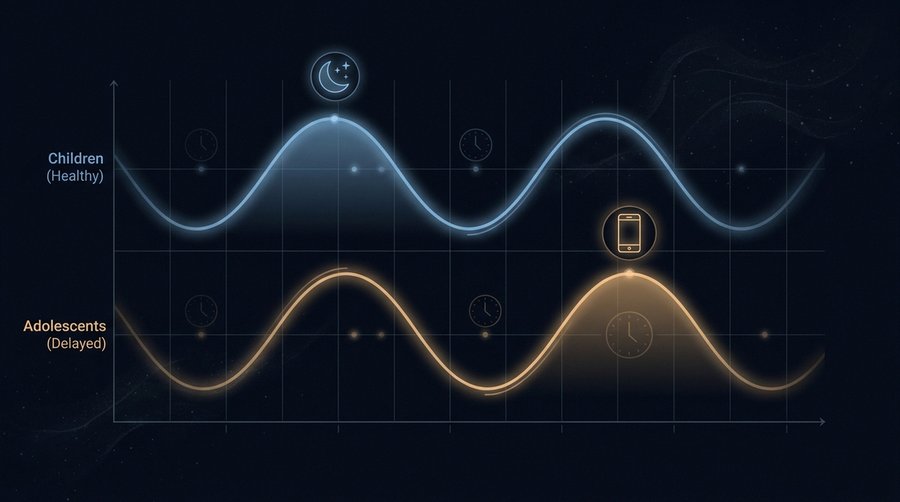
The adolescent preference for later sleep and later waking is one of the most reliably documented phenomena in sleep science, and one of the most consistently misattributed to willpower or discipline. The biological reality: puberty triggers a phase delay in the master circadian oscillator, the suprachiasmatic nucleus, that is independent of social behaviour and driven by neuroendocrine changes during sexual maturation.
Hagenauer, Perryman, Lee, and Carskadon (2009, Developmental Neuroscience, vol. 31, pp. 276–284) reviewed the cross-species evidence for pubertal sleep phase delay across six independent laboratories. Their synthesis documented a consistent 1 to 4-hour delay in circadian rhythm timing during puberty — with the peak occurring in late adolescence, around age seventeen to nineteen, before gradually advancing toward adult chronotype in the mid-twenties. In humans, the effect is sexually differentiated: males show a greater chronotype delay and a later reversal than females.
Two mechanisms drive the shift. First: reduced sensitivity of the circadian system to morning zeitgeber light during puberty, meaning the SCN anchors DLMO later because it is less responsive to morning photon input. Second: a slowing of the homeostatic sleep pressure build-up during waking hours, which extends the tolerable wake window and naturally pushes sleep onset later. Both changes are pubertal in origin, both are reversible as adolescence ends — and both are substantially worsened by evening exposure to blue-rich screen ALAN. Social jetlag — the chronic mismatch between biological sleep timing and enforced school-schedule wake time — is the daily consequence.
DSPD and Adolescent Prevalence
What most parents call a bad sleep habit meets the clinical criteria for a circadian rhythm disorder in a substantial minority of teenagers.
Delayed Sleep-Wake Phase Disorder (DSPD), classified under ICSD-3 and DSM-5, describes a chronic, stable delay in the major sleep episode relative to the conventional social schedule that cannot be corrected by an act of will. DSPD patients are not night owls with poor habits. They are people whose circadian clocks are anchored in a phase that makes physiological sleep impossible at conventional bedtimes — typically unable to sleep before 2:00 to 4:00 a.m., and correspondingly unable to wake before 10:00 to 12:00 noon without impairment.
In the general adult population, DSPD prevalence is approximately 0.17%. Among adolescents, the picture is dramatically different. Sivertsen, Pallesen, Stormark, and colleagues (2013, BMC Public Health, 13:1163) surveyed 10,220 adolescents aged 16 to 18 in Hordaland County, Norway, and found a DSPD prevalence of 3.3% using ICSD-2 criteria — nearly twenty times the adult rate. Broader estimates of clinically significant delayed phase, including sub-threshold presentations, reach 7 to 16% depending on the diagnostic criteria and population studied. Thorleifsdottir and colleagues (2002, Journal of Psychosomatic Research, 53:529–537) documented in an Icelandic longitudinal cohort that over 70% of individuals aged 16 to 21 reported frequent daytime sleepiness — a direct functional consequence of circadian misalignment.
ALAN is not the sole cause of adolescent DSPD. The pubertal chronotype shift creates the substrate; ALAN — particularly evening screen exposure in the 450 to 490 nm range — deepens and stabilises the delay. It is an exacerbating factor of the first order. And it is the most modifiable one.
Screen Time: What the Meta-Analyses Show
Ninety percent of studies in two major systematic reviews found screen time adversely associated with sleep. The effect is small to moderate but consistent across study designs.
Hale and Guan (2015, Sleep Medicine Reviews, vol. 21, pp. 50–58) systematically reviewed 67 studies on screen time and sleep in school-aged children and adolescents, covering television, computers, video games, and mobile devices. Ninety percent of studies found adverse associations between screen use and sleep outcomes, primarily shorter sleep duration and delayed bedtime. Effect sizes were small to moderate individually. Accumulated across thousands of nights, small shifts compound.
Carter, Rees, Hale, Bhattacharjee, and Paradkar (2016, JAMA Pediatrics, 170(12):1202–1208) conducted a meta-analysis of studies examining portable screen devices specifically — phones and tablets — and sleep in children and adolescents. Portable device access was associated with significantly increased odds of inadequate sleep duration (OR = 2.17; 95% CI: 1.61–2.94) and poor sleep quality (OR = 1.46; 95% CI: 1.14–1.88). Bedtime device use showed stronger associations than passive access.
Cain and Gradisar (2010, Sleep Medicine, 11(8):735–742), reviewing 36 studies on electronic media and sleep across school ages, documented the most consistent finding: later bedtime and reduced total sleep time, regardless of device type. Television watching, gaming, and internet use all showed the association; smartphones were not yet dominant in 2010 but the pattern held wherever studied.
The mechanism is layered. Blue-rich screen light suppresses melatonin via ipRGCs, directly delaying DLMO. Cognitive and emotional engagement with content extends waking arousal. Notifications interrupt sleep maintenance. These three pathways run simultaneously.
School Performance and Mental Health
Chronic adolescent sleep deprivation has measurable cognitive, emotional, and psychiatric consequences — and screen ALAN sits squarely in the causal pathway.
Chronically sleep-deprived adolescents are not merely tired. Hippocampal memory consolidation, primarily occurring in NREM slow-wave sleep, is truncated when sleep is cut short. Working memory, attention, and executive function degrade. Reaction times deteriorate. Mood regulation — dependent on both REM sleep and adequate melatonin signalling — becomes less stable. These are measurable, dose-dependent effects: each hour of lost sleep predicts specific cognitive performance decrements.
Twenge, Joiner, Rogers, and Martin (2018, Clinical Psychological Science, 6(1):3–17) found that U.S. adolescent depression and suicide-related outcomes increased markedly after 2010, correlating with increased smartphone adoption across two nationally representative surveys of over 506,000 students. The study is correlational and has attracted methodological debate — the direction of causality between depression and screen time remains contested. The sleep-mediation pathway, however, is more mechanistically established: screen ALAN delays sleep, sleep deprivation predicts depression onset, and this pathway has been replicated across multiple prospective studies. Whether screens harm mental health directly or primarily through sleep disruption is an open question. That sleep disruption harms mental health is not. For the mechanistic overlap between ALAN-driven sleep loss and psychiatric risk, see shift work, IARC Group 2A, and the cancer evidence; the melatonin-serotonin pathway is shared. Broader metabolic consequences are covered in light pollution and human health.
What Works: Practical Interventions
The evidence base supports a combination approach. Screen curfews, spectral filters, and structural solutions each do something. None is sufficient alone.
Blue light filter software — Night Shift on iOS, f.lux, Android’s adaptive display modes — reduces the short-wavelength component of screen output without eliminating screen use. Cajochen’s group at the University of Basel demonstrated measurable melatonin-suppression reduction with blue-filtered screens in controlled conditions. The effect is real but partial. Reducing blue content from a screen at full brightness still leaves substantial melanopic irradiance. The filter works better combined with reduced screen brightness in the pre-sleep window.
Red light glasses — blocking wavelengths below 530 nm — are more effective per-lux at protecting melatonin than software filters, because they act upstream at the eye rather than downstream at the source. Compliance is the limiting factor, particularly in adolescents.
Screen curfews two hours before sleep have the strongest evidence base for adolescent sleep improvement: Hale and Guan’s review found digital-free pre-sleep periods consistently associated with earlier bedtimes and longer sleep duration. Two hours matches the DLMO window — the period of maximum ipRGC sensitivity — and is the most evidence-grounded single recommendation. Difficult to enforce. That matters.
School start times are where structural solutions become visible. The American Academy of Pediatrics published a formal policy statement in 2014 (Pediatrics, 134(3):642–649) recommending that middle and high schools start no earlier than 8:30 a.m. Wheaton, Chapman, and Croft (2016, Journal of School Health, 86(5):363–370) reviewed 38 studies showing that delayed start times reliably increase weeknight sleep duration, reduce tardiness and absenteeism, and improve academic performance. Sweden’s Karolinska-linked research and Netherlands pilot programmes have reached comparable conclusions.
My position: individual interventions — app settings, glasses, bedtime rules — matter and should be used. They are not sufficient substitutes for structural solutions. A school system that requires seventeen-year-olds to perform at 7:30 a.m. is not asking adolescents to overcome a bad habit. It is asking them to override developmental biology. The policy tool exists. The AAP endorsed it in 2014. For population-level policy instruments in action, see how to reduce light pollution: engineering, policy, and ecological design.
Frequently Asked Questions
Is a screen in a child’s bedroom really harmful?
The association between bedroom screens and shorter, worse sleep is one of the most consistent findings in the paediatric sleep literature. Carter et al. (2016, JAMA Pediatrics) found device access was associated with over twice the odds of inadequate sleep duration. The harm is not linear: it depends on when and how devices are used. Bedtime use — in the two hours before sleep onset — carries the highest circadian cost because it falls exactly in the DLMO window where ipRGC sensitivity peaks and melatonin suppression is most consequential. Passive device access without bedtime use carries far less risk.
Do blue light filter glasses or Night Shift mode work?
Both reduce melatonin suppression — neither eliminates it. Night Shift and similar software filters shift the screen spectrum toward warmer wavelengths, reducing short-wavelength content by roughly 20 to 50% depending on the setting. Red or amber glasses that block below 530 nm achieve greater protection because they function regardless of device settings and screen content. A filtered screen at full brightness still delivers substantial melanopic irradiance. Filter plus reduced brightness plus a pre-sleep screen curfew outperforms any single intervention.
At what age do children’s eyes start yellowing?
Lens yellowing is a continuous process beginning in early adulthood and accelerating after age forty. In children and adolescents, the lens is largely transparent to short-wavelength light — which is exactly why they are more, not less, vulnerable to blue-light-driven melatonin suppression than adults. Kessel et al. (2011) found the 480 nm transmission rate declines by 0.7 to 0.8% per year across the lifespan. At ten years old, a child transmits roughly 85 to 90% of incoming 480 nm light to the retina — a liability for circadian health in any screen-saturated evening environment.
Should schools start later for teenagers?
Yes — the evidence is unambiguous on this point. The AAP’s 2014 policy statement recommended no earlier than 8:30 a.m. for middle and high school start times, based on a substantial body of research linking early start times to chronic sleep deprivation, impaired academic performance, elevated depression risk, and increased motor vehicle crashes in adolescent drivers. Wheaton et al.’s 2016 review of 38 studies confirmed that delayed start times increase sleep duration without evidence of proportional bedtime delay. Adolescent chronotype is phase-delayed by 1 to 4 hours — asking a sixteen-year-old to perform at 07:30 is equivalent to asking an adult to perform at 04:30.